


Women are often concerned about whether either an untreated psychiatric illness or antidepressants increase the risk of a spontaneous abortion (miscarriage). Fortunately, data are now available that are consistently reassuring and indicate that antidepressants do not increase the risk, although women who suffer from mood disorders might be at higher risk for miscarriage.
One recent large study was reported by Kjaersgaard and colleagues. This research group assessed over one million pregnancies included in the Danish Medical Birth Registry and the Danish National Hospital Registry. Data were assessed for 1,005,319 pregnancies, of which 114,721 (11.4%) ended in a spontaneous abortion. Out of the total population, 22,061 pregnancies had exposure to antidepressants and 1,843 pregnancies had mothers with a diagnosis of depression but with no antidepressant use. Miscarriage occurred in 2,637 (12.0%) of women with antidepressant exposure (12.0%) and in 205 (11.1%) of women with depression but no exposure.
Antidepressant exposure was associated with a relative risk (RR) of 1.14 (95% confidence interval (CI) 1.10-1.18) for spontaneous abortion compared with no exposure to antidepressants. This constitutes a very small but statistically significant increase in risk with antidepressant exposure. This finding is consistent with findings from Hemels and colleagues (2005) in which using data from 6 cohort studies was analyzed; antidepressant users were slightly more likely than non-depressed, non-antidepressant-exposed women to experience miscarriage.
However, it is plausible that depression itself could either directly or indirectly contribute to an increased risk of pregnancy loss. To take this into account, the authors compared women taking antidepressants to women who had diagnoses of depression but were not taking antidepressants. Among women with a diagnosis of depression, the relative risk for spontaneous abortion after any antidepressant exposure was 1.00 (95% CI 0.80-1.24). They also systematically looked at individual antidepressants. None of the SSRIs were associated with spontaneous abortions.
In unadjusted analyses, less commonly used antidepressants, such as mirtazapine, venlafaxine, and duloxetine, were associated with spontaneous abortions among women with depression. However, the number of women on these medications was much smaller, making the precision of these findings more questionable, and it is possible that patients on these medications had more severe or treatment resistant depression, considering SSRIs are often considered first-line antidepressants for use in pregnancy.
To summarize, the authors found a slightly increased risk of spontaneous abortion associated with the use of antidepressants. However, when comparing women with histories of depression, antidepressants in general, or individual SSRIs in particular, were not associated with an increased risk of spontaneous abortions. The lack of association between antidepressant use and spontaneous abortion is consistent with a rigorous meta-analysis done by Ross and colleagues (2013), who did not find a significant association.
Two graphs from this article illustrate the very thoughtful comments made by Palmsten and Hernandez-Diaz (Epidemiology 2012) regarding the difficulty in interpreting the data these sorts of studies:
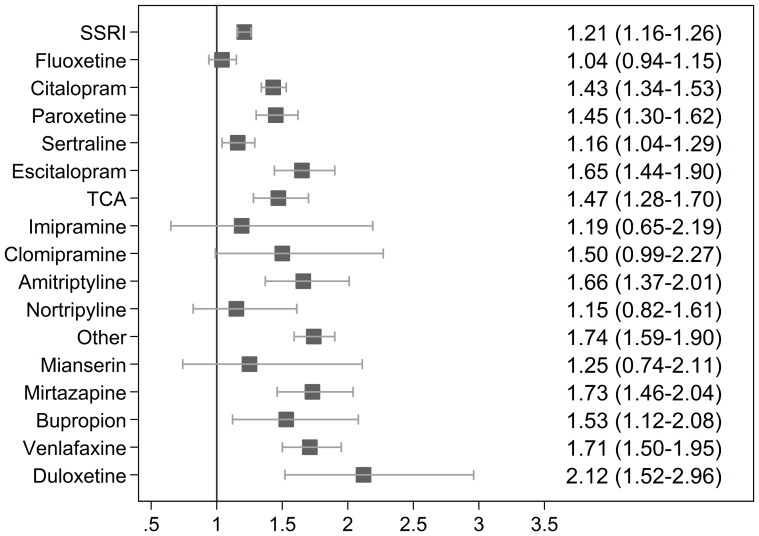
In these 2 graphs, the vertical line represents no increased risk. Squares to the right represent increased risk associated with each type of exposure. In the first graph (on the left), antidepressant users are compared to all non-antidepressant users. In the second graph (on the right), antidepressant users are compared only to women with depression who were not treated with antidepressants. What is so interesting here is that we see the squares shift to the left for the SSRIs. There is no evidence of risk when women with antidepressant use are compared to women with depression who are not using antidepressants; thus, the data looks very different when a more appropriate control group is chosen.
While reassuring about the risk of pregnancy loss and antidepressant exposure, it appears that having depression itself may impact the risk of miscarriage. Some have hypothesized that exposure to depression itself may negatively affect pregnancy outcomes. Another possible explanation is that women with depression are more likely to engage in behaviors (e.g., smoking, alcohol use, decreased use of prenatal vitamins) that may increase the risk of adverse outcomes. One limitation of this study is that the authors could not account for the severity of current and past illness for in this data base; nor did they have data on other possible confounding factors.
Marlene Freeman, MD
Kjaersgaard MI, Parner ET, Vestergaard M, et al. Prenatal antidepressant exposure and risk of spontaneous abortion – a population-based study. PLoS One. 2013 Aug 28; 8(8):e72095.







